HEALTH CARE CHALLENGES and PHARMACOECONOMICS
Over the years, the Canadian Pharmacists Association (CPHA) has worked to present what they see challenges and concerns to the various governments on Canada's Health program. The challenges have included issues regarding public education on wellness and disease, screening to detect early disease, appropriate use of drugs and development of the role of information technology in health care. Read more about the CPHA including its updated membership model and "What We Do."
Health Care Costs
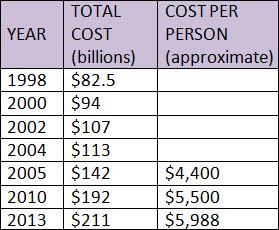
Not surprisingly health care costs under the Medicare program have steadily increased since its national adoption in the early 1960s. However, and what is an eye opener, the Health of Canadians has not increased comparably. The federal government is picking up less of the cost of health care leaving the provinces and territories scrambling to keep the system afloat. In 2004, Ontario reacted by removing coverage for routine eye examinations for adults between the ages of 20 and 64 in an effort to control costs. There are similar examples of removal of previously paid for health related services across the country.
Not only have overall health care costs ballooned in recent years, the cost per capita has followed suit as indicated in the table to the left.
Total Health Spending (Hospitals)
The graph shown here illustrates the changes in hospital spending in Canada for a 20 year time period (1983-2003). Of particular note is the reduction in inpatient nursing and staffing services while at the same time a significant increase in ambulatory services (e.g. day surgeries) and diagnostic services. In practical terms patients are now sent home from hospital "quicker and sicker" while many support staff positions (e.g. housekeeping, grounds keeping) have been contracted out resulting in a net savings to the hospital. Diagnostic expenses have increased in large part to the widespread use of new expensive technologies such as Magnetic Resonance Imaging (MRI) machines.
Distribution of Health Spending
This pie chart shows the breakdown of health spending in various areas including retail drugs, physician services, public health and hospitals. As you can see, expenditures on hospitals at 30% of the total far exceeded that of any other category in 2005. Compare the information in this chart from 2011. Which categories have changed? Which ones have stayed relatively the same?
Cost-Related Access Problems
Compare the information shown here regarding filling prescription drugs, visiting the doctor and attending follow-up appointments by country. In particular, compare the statistics shown for Canada and the United States. Why do you think Canadians appear more "compliant" when it comes to health care?
Canadians and Prescription Drugs
Drug spending in Canada has increased significantly. Compare the average cost per person of $3.80 spent per month on prescription drugs in 1985, $30.00 per month in 2008 and $55.00 per month in 2013. Not only have the number of prescription drugs filled and taken by Canadians increased but the cost of those drugs have also increased. New to the market drugs in particular are often very expensive allowing for drug manufacturers to recoup the money they invested in research. However, just because a drug is new does not necessarily make it more effective. Increasing professional fees and drug mark ups have added to the increase in the cost of prescriptions drugs.
There is also a trend toward drug therapies versus other types of treatment or none at all (e.g. the use of Viagra for Erectile Dysfunction). At the same time, the prescribing habits of physicians has changed. Physicians are writing more prescriptions (and for larger quantities) than ever often at the insistence of patients (e.g. parents demanding antibiotics for a child with a virus). It has been argued that too many drugs are being prescribed sometimes causing more harm than good as in the case of antibiotic resistant bacteria.
Canada Health and Social Transfer (CHST)
In 1996/97 the federal government’s contribution to provincial health and social programs was consolidated into a new single block transfer only to be split again in 2004 into the Canada Health Transfer (CHT) and the Canada Social Transfer (CST). This was done in order to provide greater "accountability and transparency" of where the money was spent. Federal funding is transferred to provinces as a combination of cash contribution and tax points. Transfer funds are tied to the province by adhering to the principles of the Canada Health Act. Funding has been held back from provinces who failed to abide by the Act.
User Fees
Do “user fees” contravene the Canada Health Act and create a “Two-tiered” system? By that we mean, one in which those who have the money can pay for a different (better?) experience with our health care system. A document produced by the Ontario Health Coalition in March of this year describes how certain private clinics are essentially getting away with charging extra fees for such things as jumping the queue to be seen by a health care provider sooner. Other facilities, and many physicians, offer "specialized" services, such as a sick note for work or school, for a fee charged to the patient of course.
Physicians in some European countries receive a flat salary based on seniority or the number of patients in their roster. In Canada, doctors bill "Fee-For-Service" encouraging multiple doctor visits. Perhaps it is time to rethink our system or reinforce it.
Healing the Health Care System
Ottawa has said that money alone will not heal our health care system. In 2002, the Royal Commission on the Future of Health Care in Canada led by Roy Romanow was completed and delivered to the government of Canada. The report contained 47 recommendations. In it Romanow identified that pharmacists could take a heightened leadership role in drug management and proposed that a national Pharmacare program should be debated. In creating the report, Romanow crossed the country and challenged Canadians to discuss their vision of health care by holding town hall meetings. He proposed 5 specific funds be designated by the government, including a Rural and remote access fund, Diagnostic services fund, Primary health care transfer fund, Home care transfer fund, and a Catastrophic drug transfer fund.
Reforming the Health Care System
As mentioned earlier, funding for health care in Canada is being squeezed. A reactionary measure of the provinces has been to devise ways in which to save money, including:
Restructuring by Hospital closures, Downsizing of beds and Implementing regional governance Rationalization of Services by Reducing duplication of medical, administration and support services Redirection of Resources from Institutional to Community based care, Focusing on health promotion and Illness prevention Integration of Related Services under a common administration (e.g. Ministry of Health AND Long Term Care) Expansion of the Home Care Sector to accommodate for post-op and continuing care in the home versus the hospital
Pharmacoeconomics
Pharmacoeconomics is a branch of health economics in which analytical methods are used to identify, measure and compare the costs and consequences of pharmacy products and services. It assists in decision making for program funding such as which drugs and/or drug products to include in the Ontario Drug Benefit Formulary. Pharmacoeconomics also provides for informed decision making on drug use policies, clinical practice guidelines, reimbursement procedures, and individual patient therapies. It is used to compare the costs and consequences of two or more competing products, services or programs and to help select an alternative drug therapy that will be funded and implemented.
CHECKPOINT Question ONE: Visit the Canadian Institute for Health Information (CIHI). At the bottom of the page, check out "What's the story in your...." province, city and a hospital that you are familiar with. Results will appear in areas of access, quality, health outcomes, spending, etc. Compare different provinces to Ontario. How are we doing?
Over the years, the Canadian Pharmacists Association (CPHA) has worked to present what they see challenges and concerns to the various governments on Canada's Health program. The challenges have included issues regarding public education on wellness and disease, screening to detect early disease, appropriate use of drugs and development of the role of information technology in health care. Read more about the CPHA including its updated membership model and "What We Do."
Health Care Costs
Not surprisingly health care costs under the Medicare program have steadily increased since its national adoption in the early 1960s. However, and what is an eye opener, the Health of Canadians has not increased comparably. The federal government is picking up less of the cost of health care leaving the provinces and territories scrambling to keep the system afloat. In 2004, Ontario reacted by removing coverage for routine eye examinations for adults between the ages of 20 and 64 in an effort to control costs. There are similar examples of removal of previously paid for health related services across the country.
Not only have overall health care costs ballooned in recent years, the cost per capita has followed suit as indicated in the table to the left.
Total Health Spending (Hospitals)
The graph shown here illustrates the changes in hospital spending in Canada for a 20 year time period (1983-2003). Of particular note is the reduction in inpatient nursing and staffing services while at the same time a significant increase in ambulatory services (e.g. day surgeries) and diagnostic services. In practical terms patients are now sent home from hospital "quicker and sicker" while many support staff positions (e.g. housekeeping, grounds keeping) have been contracted out resulting in a net savings to the hospital. Diagnostic expenses have increased in large part to the widespread use of new expensive technologies such as Magnetic Resonance Imaging (MRI) machines.
Distribution of Health Spending
This pie chart shows the breakdown of health spending in various areas including retail drugs, physician services, public health and hospitals. As you can see, expenditures on hospitals at 30% of the total far exceeded that of any other category in 2005. Compare the information in this chart from 2011. Which categories have changed? Which ones have stayed relatively the same?
Cost-Related Access Problems
Compare the information shown here regarding filling prescription drugs, visiting the doctor and attending follow-up appointments by country. In particular, compare the statistics shown for Canada and the United States. Why do you think Canadians appear more "compliant" when it comes to health care?
Canadians and Prescription Drugs
Drug spending in Canada has increased significantly. Compare the average cost per person of $3.80 spent per month on prescription drugs in 1985, $30.00 per month in 2008 and $55.00 per month in 2013. Not only have the number of prescription drugs filled and taken by Canadians increased but the cost of those drugs have also increased. New to the market drugs in particular are often very expensive allowing for drug manufacturers to recoup the money they invested in research. However, just because a drug is new does not necessarily make it more effective. Increasing professional fees and drug mark ups have added to the increase in the cost of prescriptions drugs.
There is also a trend toward drug therapies versus other types of treatment or none at all (e.g. the use of Viagra for Erectile Dysfunction). At the same time, the prescribing habits of physicians has changed. Physicians are writing more prescriptions (and for larger quantities) than ever often at the insistence of patients (e.g. parents demanding antibiotics for a child with a virus). It has been argued that too many drugs are being prescribed sometimes causing more harm than good as in the case of antibiotic resistant bacteria.
Canada Health and Social Transfer (CHST)
In 1996/97 the federal government’s contribution to provincial health and social programs was consolidated into a new single block transfer only to be split again in 2004 into the Canada Health Transfer (CHT) and the Canada Social Transfer (CST). This was done in order to provide greater "accountability and transparency" of where the money was spent. Federal funding is transferred to provinces as a combination of cash contribution and tax points. Transfer funds are tied to the province by adhering to the principles of the Canada Health Act. Funding has been held back from provinces who failed to abide by the Act.
User Fees
Do “user fees” contravene the Canada Health Act and create a “Two-tiered” system? By that we mean, one in which those who have the money can pay for a different (better?) experience with our health care system. A document produced by the Ontario Health Coalition in March of this year describes how certain private clinics are essentially getting away with charging extra fees for such things as jumping the queue to be seen by a health care provider sooner. Other facilities, and many physicians, offer "specialized" services, such as a sick note for work or school, for a fee charged to the patient of course.
Physicians in some European countries receive a flat salary based on seniority or the number of patients in their roster. In Canada, doctors bill "Fee-For-Service" encouraging multiple doctor visits. Perhaps it is time to rethink our system or reinforce it.
Healing the Health Care System
Ottawa has said that money alone will not heal our health care system. In 2002, the Royal Commission on the Future of Health Care in Canada led by Roy Romanow was completed and delivered to the government of Canada. The report contained 47 recommendations. In it Romanow identified that pharmacists could take a heightened leadership role in drug management and proposed that a national Pharmacare program should be debated. In creating the report, Romanow crossed the country and challenged Canadians to discuss their vision of health care by holding town hall meetings. He proposed 5 specific funds be designated by the government, including a Rural and remote access fund, Diagnostic services fund, Primary health care transfer fund, Home care transfer fund, and a Catastrophic drug transfer fund.
Reforming the Health Care System
As mentioned earlier, funding for health care in Canada is being squeezed. A reactionary measure of the provinces has been to devise ways in which to save money, including:
Restructuring by Hospital closures, Downsizing of beds and Implementing regional governance Rationalization of Services by Reducing duplication of medical, administration and support services Redirection of Resources from Institutional to Community based care, Focusing on health promotion and Illness prevention Integration of Related Services under a common administration (e.g. Ministry of Health AND Long Term Care) Expansion of the Home Care Sector to accommodate for post-op and continuing care in the home versus the hospital
Pharmacoeconomics
Pharmacoeconomics is a branch of health economics in which analytical methods are used to identify, measure and compare the costs and consequences of pharmacy products and services. It assists in decision making for program funding such as which drugs and/or drug products to include in the Ontario Drug Benefit Formulary. Pharmacoeconomics also provides for informed decision making on drug use policies, clinical practice guidelines, reimbursement procedures, and individual patient therapies. It is used to compare the costs and consequences of two or more competing products, services or programs and to help select an alternative drug therapy that will be funded and implemented.
CHECKPOINT Question ONE: Visit the Canadian Institute for Health Information (CIHI). At the bottom of the page, check out "What's the story in your...." province, city and a hospital that you are familiar with. Results will appear in areas of access, quality, health outcomes, spending, etc. Compare different provinces to Ontario. How are we doing?

{kind=link}
{kind=link}
{kind=link}
{kind=link}